Vitiligo Surgery :
What is vitiligo?
Vitiligo is a chronic skin disorder that causes areas of skin to lose colour. The disease has a major impact on the quality of life of patients, particularly the Indian population, in which there is a severe stigma attached to the disease. Due to these effects, there is a considerable need for active treatment of this disease.
Who are the ideal candidates for vitiligo surgery?
Certain types of vitiligo do not respond well to medical treatment and resistant lesions do persist even in those who respond. The stability status of vitiligo is the single most important prerequisite in case selection. It work best for patients with stable vitiligo (patients that have no new lesions or no further progression of the condition over last 1 years)
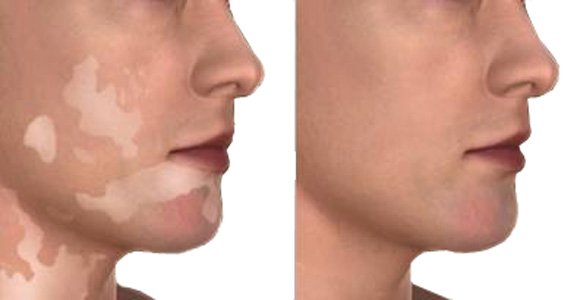
Goal of vitiligo surgery?
The goal of vitiligo surgery is to achieve complete repigmentation of the affected area that cosmetically matches with the surrounding normal skin.
Types of vitiligo surgery:
All types of surgical treatment aim to transfer melanocytes (pigment-producing cells) from normal skin (the donor site) to the skin affected by vitiligo under local anaesthesia . After a few months, the transplanted melanocytes start working to make pigment, which deposits in the surrounding skin and the white spots disappear.
Surgical treatment for vitiligo can be considered in two main categories:
Grafting of melanocyte-rich tissue (tissue grafting)
Grafting of melanocyte cells (cellular grafting)
Grafting of melanocyte-rich tissue
1)Miniature punch grafting:
Miniature punch grafting is one of the most commonly used techniques. Bits of skin about 1-2 mm in diameter are punched out from the donor site on buttock or thigh and placed on the donor site of vitiliginous skin, where recipient chambers have also been created by punches.
This is the easiest and least expensive method but it is not suitable for large lesions and it can cause cobblestoning and a polka dot appearance at the recipient area
2)Suction blister grafting:
This procedure consists of obtaining very thin skin grafts consisting of only the epidermis.
In suction blister grafting, negative pressure is applied to the normally pigmented donor site to promote the formation of multiple blisters. The roofs of the blisters (the grafts) are surgically removed and transplanted onto the prepared recipient site.
It yields excellent cosmetic results with least chances of scarring at the donor as well as the recipient sites. This procedure is time consuming and large areas can not be treated by this method.
3)Split thickness skin grafting:
Split thickness skin grafting involves shaving off thin layers of skin from the donor site. In comparison to the above methods, split thickness skin grafting can cover larger areas and produces uniform pigmentation. Disadvantages are 'stuck-on' appearance of the graft, curling of the border withbeaded appearance, color mismatch, donor site scarring.
Grafting of melanocyte cell suspensions
1)Autologous non-cultured epidermal cell suspensions:
This method is now considered as the treatment of choice for surgical management of vitiligo. Tissue is harvested from a donor site and is incubated with enzyme solution to separate the epidermis from the dermis. The melanocytes(the colour giving cells) are then separated from the epidermis and made into a cell suspension that can then be transplanted onto the de-epithelialized recipient skin.
Autologous non-cultured epidermal cell suspensions allow large areas to be treated in one session using a small donor graft, with the donor-to-recipient expansion ratio ranging from 5-10 fold. They result in excellent colour matching
2)Cultured melanocyte suspensions:
Tissue harvested from the donor sites are incubated with trypsin. Melanocytes and keratinocytes are then separated from the epidermis and are incubated in a medium that contains growth factors. After culturing, the suspension is transplanted to the recipient sites. This sophisticated technique requires a special laboratory.